Angioimmunoblastic T-Cell Lymphoma (AILT/AILD)
You are here
We are missing a sample case. If you have one, please attach it, or contact us and we will help post it.
Definition
Angioimmunoblastic T-cell lymphoma (AILT/AILD) is a mature T-cell lymphoma with systemic characterized by a polymorphous lymph node infiltrate showing a marked increase in follicular dendritic cells (FDCs), high endothelial venules (HEVs) and systemic involvement. It is also known as immunoblastic lymphadenopathy (Lukes-Collins Classification) and AILD-type (lymphogranulomatosis X) T-cell lymphoma (Kiel Classification).
Epidemiology
The typical patient with angioimmunoblastic T-cell lymphoma (AILT/AILD) is either middle-aged or elderly, and no gender preference for this disease has been observed. AILT/AILD comprises 15-20% of peripheral T-cell lymphomas and 1-2% of all non-Hodgkin lymphomas.
Possible causes
This disease was originally thought to be a premalignant condition, termed angioimmunoblastic lymphadenopathy, and this atypical reactive lymphadenopathy carried a risk for transformation into a lymphoma. Currently, it is postulated that the originating cell for this disease is a mature (post-thymic) CD4+ T-cell that arises de novo, although some researchers argue that there is a premalignant subtype of this disease. The Epstein Barr virus (EBV) is observed in the majority of cases, and the virus has been found in the reactive B-cells that comprise part of the polymorphous infiltrate of this disease and in the neoplastic T-cells. Immunodeficiency is also seen with this disease, but it is thought to be a sequela to the condition and not a predisposing factor.
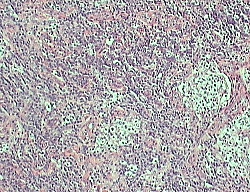
Morphology
Lymph node: The normal architecture of a lymph node is partially effaced by a polymorphous infiltrate and residual follicles are commonly seen. The polymorphous infiltrate consists of lymphocytes of moderate size with pale/clear cytoplasm and smaller reactive lymphocytes, eosinophils, histiocytes, plasma cells, and follicular dendritic cells. In addition, blast-like B-cells are occasionally seen. A classic morphological finding is the aborization and proliferation of high endothelial venules. Hyperplastic germinal centers and Reed-Sternberg cells can also be seen.
The cytological spectrum of atypical lymphocytes is extremely broad: small to large-sized cells with often regular or indented nuclei, moderately condensed chromatin, moderate to faint basophilic cytoplasm without azurophilic granules and sometimes with microvacuoles.
 |
Immunophenotyping
These mature T-lymphoid cells express a mixed CD4/CD8 expression (CD4 usually outnumber CD8). Aberrant T cell antigen expression is common, most often with loss of CD3 and/or CD7. The fluorescent expression of T cells is much dimmer than it's benign counterparts. The majority of AILT/AILD cell coexpress T cells markers and CD10. Plasma cells, if present, are polyclonal. Follicular Dendridic cells (FDCs) are CD21+ and conspicuous. bcl-6 may also be positive.
Other relevant tests
Genetics: Clonal T-cell receptor gene rearrangements are detected in 75% of cases, and immunoglobin gene rearrangements are seen in 10% of cases, and these cases are believed to be due to expanded EBV-driven B-cell populations. Similarly, EBV-related sequences can be detected most cases, usually in B-cells but occasionally in T-cells. Trisomy 3, trisomy 5, and +X are the most frequent chromosomal abnormalities found in cases.
Flow Diagnosis
These mature T-lymphoid cells express a mixed CD4/CD8 expression (CD4 usually outnumber CD8). Aberrant T cell antigen expression is common, most often with loss of CD3 and/or CD7. The fluorescent expression of T cells is much dimmer than it's benign counterparts. The majority of AILT/AILD cell coexpress T cells markers and CD10. Plasma cells, if present, are polyclonal. Follicular Dendridic cells (FDCs) are CD21+ and conspicuous. bcl-6 may also be positive.
References
Weiss LM, Jaffe ES, Liu XF, Chen YY, Shibata D, Medeiros LJ. "Detection and localization of Epstein-Barr viral genomes in angioimmunoblastic lymphadenopathy and angioimmunoblastic lymphadenopathy-like lymphoma." Blood. 1992 Apr 1;79(7):1789-95. PMID: 1373088
Siegert W, Nerl C, Agthe A, Engelhard M, Brittinger G, Tiemann M, Lennert K, Huhn D. "Angioimmunoblastic lymphadenopathy (AILD)-type T-cell lymphoma: prognostic impact of clinical observations and laboratory findings at presentation. The Kiel Lymphoma Study Group." Ann Oncol. 1995 Sep;6(7):659-64. PMID: 8664186
Anagnostopoulos I, Hummel M, Finn T, Tiemann M, Korbjuhn P, Dimmler C, Gatter K, Dallenbach F, Parwaresch MR, Stein H. "Heterogeneous Epstein-Barr virus infection patterns in peripheral T-cell lymphoma of angioimmunoblastic lymphadenopathy type." Blood. 1992 Oct 1;80(7):1804-12. PMID: 1327284
Sample Cases
Click here for instructions on how to download the free FCS Express Reader to view and manipulate the sample cases.