Acute T Lymphoblastic Leukemia/Lymphoma (T ALL)
You are here
Definition
(T-ALL) is a type of acute lymphoblastic leukemia (ALL), a cancer of the lymphocyte-forming cells called lymphoblasts. T-ALL is a neoplasm where blasts have committed to the T lineage.
Sample Cases
Click here for instructions on how to download the free FCS Express Reader to view and manipulate the sample cases.
| Case Name (click on case name to open) |
Comments | Size |
| T-ALL1 |
T-ALL with CD30 |
5Mb |
| T-ALL2 |
T-ALL |
4 Mb |
| T Cell ALL | T Cell ALL case submitted by UTMC. Normal PB for reference. | 2 Mb |
Epidemiology
About 13% to 15% of children with ALL have T-cell ALL. This type of leukemia affects boys more than girls, and generally affects children at an older age than B-cell ALL does. It is often associated with an enlarged thymus (which can sometimes cause breathing difficulty) and with early spread to the cerebrospinal fluid (the fluid that surrounds the brain and spinal cord).
Possible causes
The aetiology of T-ALL is basically unknown, It has been suggested to be caused by a defect in the Notch signaling pathway.
Morphology
Morphologically, T lymphoblasts are similar to B lymphoblasts in B ALL. They are medium-sized with scanty, often eccentric cytoplasm which occasionally creates a "mirror-hand" appearance. Chromatin is fine and nucleoli are present but inconspicuous. Presence of mitiotic figures in more prevalent in T ALL.
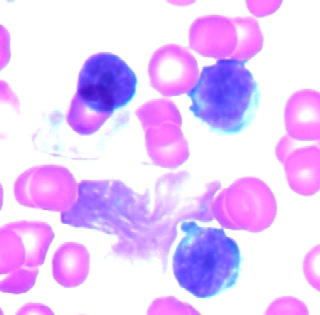 |
| Example morphology of T ALL blast. |
WHO classification
The recent WHO International panel on ALL recommends that the FAB morphologic classification (L1, L2, L3) be abandoned, since this classification has no clinical or prognostic relevance. It instead advocates the use of the immunophenotypic classification. There are 2 main immunologic types: pre-B cell and pre-T cell.
Immunophenotyping
Blasts in T ALL can be initially identified using a SSC vs CD45 plot. These blasts have low SSC (many times smaller than normal lymphocytes) and dim to negative CD45. This differs from AML where the SSC is higher.
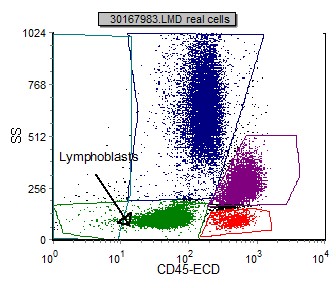 |
| T ALL blast location on CD45 vs SSC gating plot. |
Immunophenotypic Markers used to identify and subclassify T-ALL and their frequency:
| CD2 | 65% |
| CD3 | 31% |
| CD5 | 88% |
| CD7 | 98% |
| CD1a | 31% |
| CD4 | 10% |
| CD8 | 8% |
| CD4+/CD8+ | 39% |
| CD4-/CD8- | 43% |
| CD10 | 24% |
| CD11b | 4% |
| CD11c | 0% |
| CD13 | 16% |
| CD33 | 19% |
| CD34 | 39% |
| CD45 (mod-bright) | 72% |
| CD45 (dim) | 27% |
| CD56 | 21% |
| CD117 | 11% |
| HLA Dr | 10% |
| TCRab | 29% |
| TCRgd | 16% |
| TCR- | 56% |
| TdT | 86% |
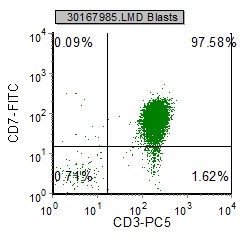
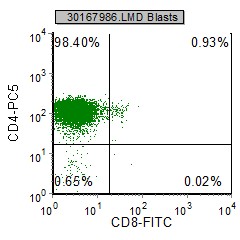
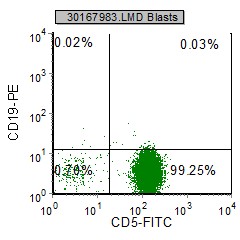
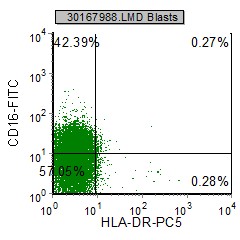
Selected example histograms in a T-ALL case:
 |
 |
 |
 |
| The blasts express the T cell markers CD3, CD5 and CD7. The B cell marker CD19 is absent. |
HLA Dr is characteristically negative |
Other relevant tests
Cytochemistry: Acid phophatase is frequently positive and localized.
Genetics: About one third of T ALL cases have translocations detected which involve the alpha and beta TCR at 14q11.2;
the beta loci at 7q35, and the gamma loci at 7p14-15. There is currently no specified clinical significance.