Mantle Cell Lymphoma (MCL)
You are here
Definition
MCL is a subtype of B-cell lymphoma, due to CD5 positive antigen-naive pregerminal center B-cell within the mantle zone that surrounds normal germinal center follicles. In addition, the cells do not die as they should and therefore accumulate in the lymphoid system, including lymph nodes and the spleen, with non-useful cells eventually rendering the system dysfunctional.
Sample Cases
Click here for instructions on how to download the free FCS Express Reader to view and manipulate the sample cases.
| Case Name (click on case name to open) |
Comments | Size |
| MCL1 | MCL | 5.1 MB |
| MCL2 | MCL with myeloid antigens | 5.1 MB |
| case 07 | MCL| This case was kindly provided by the ASCP Press. It is part of Flow Cytometry in Clinical Diagnosis by John Carey, Phil McCoy and David Keren. |
2.83 MB |
| case 38 | MCL| This case was kindly provided by the ASCP Press. It is part of Flow Cytometry in Clinical Diagnosis by John Carey, Phil McCoy and David Keren. |
629 kB |
| MCL3 | Classic MCL submitted by UTMC. | 1.52 MB |
Epidemiology
Mantle cell lymphoma (MCL) is one of the rarer of the non-Hodgkin's lymphomas, comprising about 6% of NHL cases. There are only about 15,000 patients presently in the U.S. (The prevalence seems to be somewhat higher in Europe.) While it is difficult to treat and seldom considered cured, investigations into better treatments are actively pursued world-wide. Median survival times were about 3 years, but are now estimated as approaching 6 years for new patients.
Possible causes
The cause is unknown and not genetic.
Morphology
MCL affected cells proliferate in a nodular or diffuse pattern with two main cytologic variants: typical or blastic. Typical cases are small to intermediate sized cells with irregular nuclei. Blastic (aka blastoid) variants have intermediate to large sized cells with finely dispersed chromatin and are more aggressive in nature.
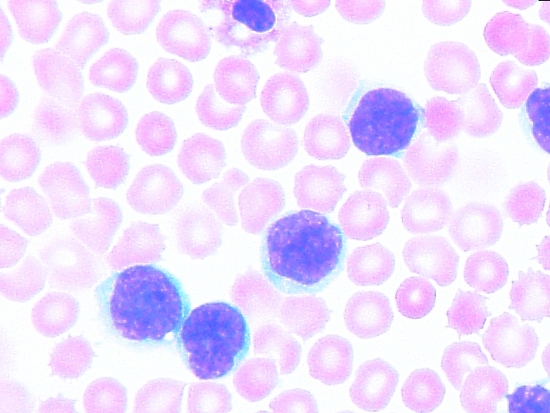 |
| Example morphology of MCL in peripheral blood. |
Immunophenotyping
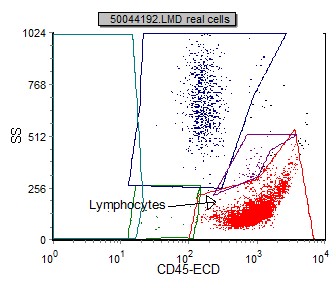
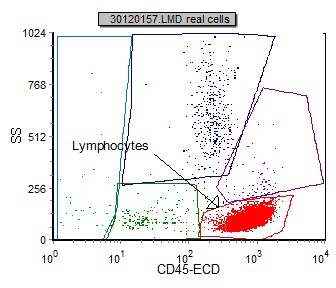
The initial gating dot plot identifies a predominant CD45 bright SSC low population consistent with lymphocytes. MCL cells fall in the lymphocyte region.
 |
 |
Immunophenotypic markers used to identify and classify MCL:
| Markers | Reaction in MCL |
| CD5 | +/rarely- |
| CD10 | -/rarely+ |
| CD20 | +(moderate) |
| CD23 | - /rarely+ |
| CD25 | - |
| CD30 | - |
| CD45 | + |
| CD103 | - |
| CD138 | - |
| bcl-1 | + |
| bcl-2 | + |
| bcl-6 | - |
| Heavy chain (IgG, IgA, IgM) | + |
| Light chain Ig (kappa or lambda) | +(moderate expression) |
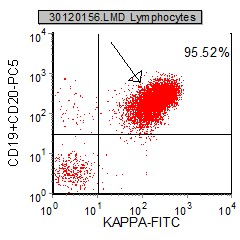
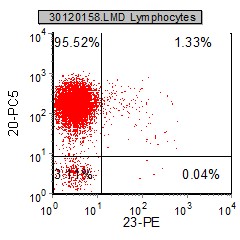
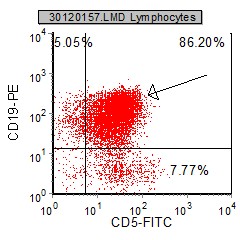
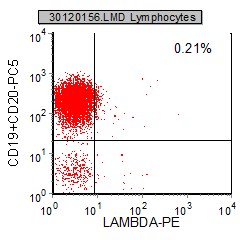
Selected example histograms from a MCL case:
 |
 |
 |
 |
 |
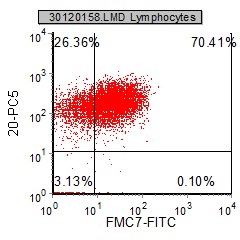 |
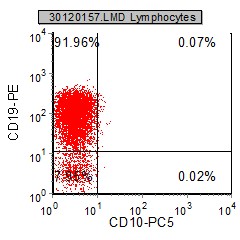
| CD19 and CD5 characteristically are expressed in MCL. CD10 is generally negative | In this case a monoclonal kappa population is identified. MCL sIg are moderatly expressed. | CD23 is caracteristically negative on MCL. FMC-7 and CD20 are expressed. CD20 is generally brighter than CD19 in MCL. |
Other relevant tests
Cytochemistry: OCT 2 and PAX-5 by immunohistochemistry are expressed in MCL.
Genetics: MCL cells generally over-express cyclin D1 due to a t(11:14) chromosomal translocation in the DNA. The cause is unknown and not genetic. MCL is not communicable. It essentially is an abnormal break and subsequent translocation in a gene that causes the cells to divide too early before becoming capable of helping to fight diseases.
Sub-classification
Morphologic varants of MCL include: blastoid, pleomorphic, small, or cells resembling MZL or monocytoid cells.
Flow Diagnosis
MCL neoplasia express monoclonal B surface light chains (kappa or lambda) and heavy chains (IgM+/-IgD). They are CD5, FMC-7 and CD43 positive . CD23 and CD10 are negative. The B cell markers CD19 and CD20 are expressed; CD20 is generally brighter than CD19 (unlike CLL). In addition the surface light chain expression is moderate.